
Meniscus Injury
An injury to the meniscus is one of the most common knee injuries. This small piece of cartilage is crucial to the pain free operation of the knee joint.
What is the Meniscus?
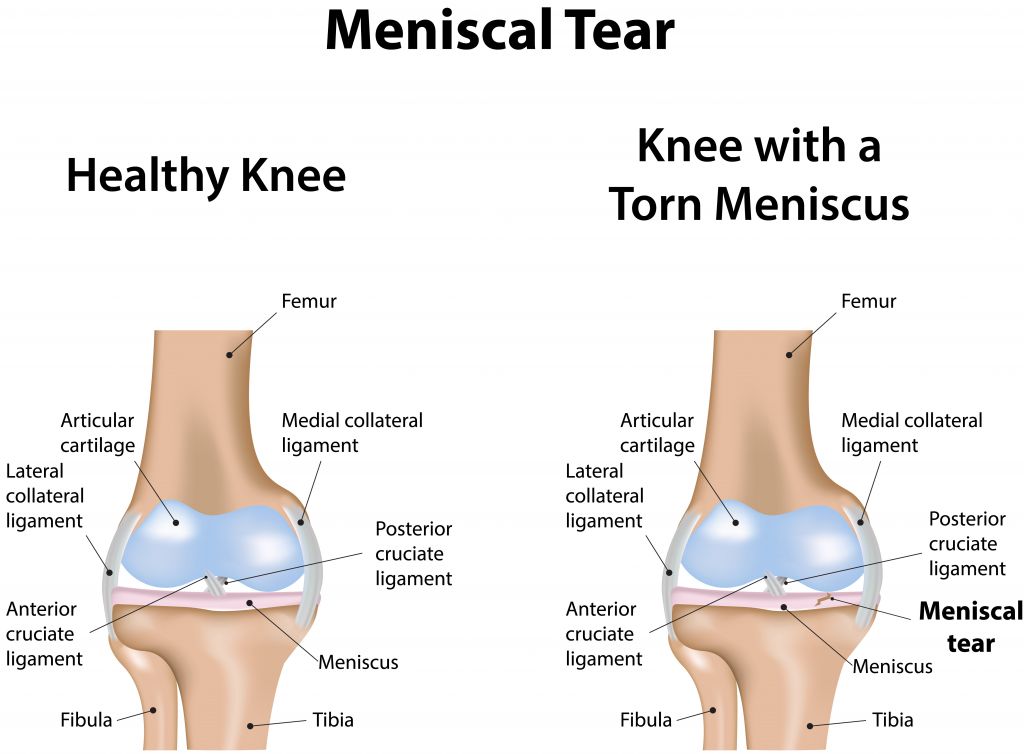
The meniscus is a disc like structure built from cartilage which is found in the middle area of the knee between the knee bones known as the femur and the tibia. There are two divisions of the meniscus, one on the (medial) inside of the knee closer to the midline of the body and one on the (lateral) outside of the knee closer to the arms. The medial meniscus is C shaped while the lateral meniscus is more circular shaped. The meniscus is a key structure for knee function and overall stability of the knee. It is a flexible structure which adapts to stresses placed on the knee.
What does the meniscus do?
The primary job of the meniscus is to help bear the weight of the body through the knee. It does this by changing shape in response to load in order to disperse the force placed on the knee. The meniscus reacts to changes from activities such as walking or climbing chairs. The meniscus also deepens the surface where the bones touch in order to increase the stability of the knee.
What does it mean to have a meniscus injury?
A meniscal tear or rupture is an injury of the meniscus caused by activity such as planting the leg and over rotating the knee. The meniscus can also be damaged by trauma such as sports or motor vehicle collision. With age, the meniscus degenerates and becomes less flexible and more vulnerable to injury. Older people may injure their meniscus without a memorable cause, often due to degeneration and prolonged use. Meniscus injury symptoms may develop over time or immediately after an injury.
Signs and symptoms of a meniscus injury may include:
- Clicking when moving the knee
- Locking of the knee
- Pain and tenderness over the mensicus
- Decreased range of motion of the knee
- Significant difficulty with kneeling and squatting
Who is most at risk?
Many people think that athletes and other active people are most at risk for meniscus injury, however, people from all different age groups and activity levels may injure the mensicus. People over 50 years may have increased risk for deterioration of the meniscus leading to damage. It is unusual for children under 10 to have a meniscus injury. People who aggressively train and play high impact sports are at a higher risk. Males are more likely to have a meniscus injury than females overall. Being overweight, having reduced leg muscle strength and having unusual leg alignments increase risk of meniscus injuries.
What are the treatment options?
There are a large percentage of people who have meniscus injuries and never develop symptoms. The majority of people with meniscus injuries are able to fully recover function and eliminate pain. A majority of meniscus injuries can be rehabilitated with proper exercise and strengthening of the leg muscles which help compensate for the meniscus injury. Using ice and anti-inflammatory medication can help reduce pain in the short term. The use of therapeutic ultrasound may aid with meniscus recovery. Maintaining strong cardiovascular health with exercises such as bike riding can aid in recovery of a meniscus injury. By extension, maintaining a healthy weight also assists in recovery. A light and comfortable knee brace may help some people with a meniscus injury. More complicated or severe meniscus injures may require surgery if conservative therapy is ineffective. Surgical procedures may be used to repair, remove or remodel different portions of the meniscus to improve knee function and decrease pain. This is typically a last resort intervention as removing portions of the meniscus increases risk of developing other knee problems in the future.
References:
Ballas, Elissa R., and Charles A. Stillman. “Anterior cruciate ligament injury and bucket handle tear of the medial meniscus.” Journal of Orthopaedic & Sports Physical Therapy 39.10 (2009): 766-766.
Hede, A., Jensen, D. B., Blyme, P., & Sonne-Holm, S. (1990). Epidemiology of meniscal lesions in the knee: 1,215 open operations in Copenhagen 1982-84.Acta orthopaedica Scandinavica, 61(5), 435-437.
Hegedus EJ, Cook C, Hasselblad V, Goode A, McCrory DC. (2007)Physical examination tests for assessing a torn meniscus in the knee: a systematic review with meta-analysis. Journal of Orthopaedic and Sports Physical Therapy, 37(9), 541-5
Meniscectomy Hwa-Jae Jeong, MD, Seung-Hee Lee, MD and Chun-Suk Ko, MD Knee Surg Relat Res 2012;24(3):129-136
Noble J, Hamblen DL (1975) The pathology of the degenerate meniscus lesion. J Bone Joint Surg Br 57:180–186
Simon C et al. Treatment of meniscal tears: An evidence based approach. World Journal of Orthopedics. Juli 2014. 5(3): 233-241
Zanetti M, Pfirrmann CW, Schmid MR, Romero J, Seifert B, Hodler J (2003) Patients with suspected meniscal tears: prevalence of abnormalities seen on MRI of 100 symptomatic and 100 contralateral asymptomatic knees. AJR Am J Roentgenol 181:635–641
Sigurdsson U, Delayed gadolinium-enhanced MRI of meniscus (dGEMRIM) and cartilage (dGEMRIC) in healthy knees and in knees with different stages of meniscus pathology, BMC Musculoskelet Disord, 2016 Sep 29.